Oncologic Emergencies
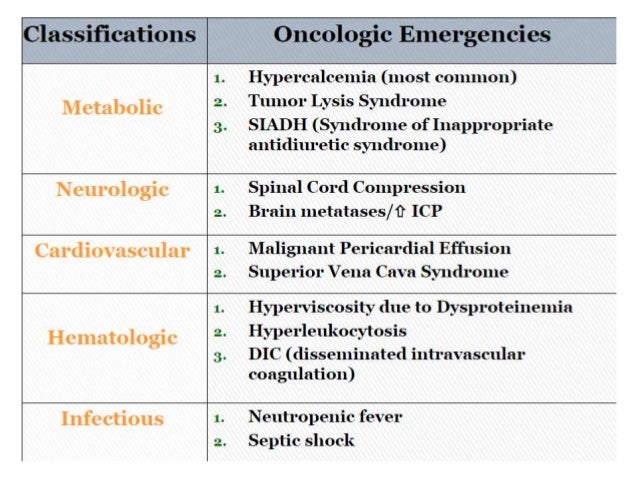 Most oncologic emergencies can be classified as metabolic, hematologic, structural, or treatment related. Tumor lysis syndrome is a metabolic emergency that presents as severe electrolyte abnormalities. Stabilization is focused on vigorous rehydration, maintaining urine output, and lowering uric acid levels. Hypercalcemia of malignancy, which is associated with poor outcomes, is treated with aggressive rehydration, intravenous bisphosphonates, and subspecialty consultation. Syndrome of inappropriate antidiuretic hormone should be suspected if a patient with cancer has hyponatremia. This metabolic condition is treated with fluid restriction or hypertonic saline, depending on the speed of development. Febrile neutropenia is one of the most common complications related to cancer treatment, particularly chemotherapy. It usually requires inpatient therapy with rapid administration of empiric antibiotics. Hyperviscosity syndrome may present as spontaneous bleeding and neurologic deficits, and is usually associated with Waldenström macroglobulinemia. Treatment includes plasmapheresis followed by targeted chemotherapy. Structural oncologic emergencies are caused by direct compression of nontumor structures by metastatic disease. Superior vena cava syndrome presents as facial edema with development of collateral venous circulation. Intravascular stenting leads to superior patient outcomes and is used in addition to oncology-directed chemotherapy and radiation therapy. Malignant epidural spinal cord compression is managed in conjunction with neurosurgery, but it is classically treated using steroids and/or surgery and radiation therapy. Malignant pericardial effusion may be treated with pericardiocentesis or a more permanent surgical intervention. Complications of cancer treatment are becoming more varied because of the use of standard and newer immunologic therapies. Palliative care is increasingly appropriate as a part of the team approach for treating patients with cancer.
Most oncologic emergencies can be classified as metabolic, hematologic, structural, or treatment related. Tumor lysis syndrome is a metabolic emergency that presents as severe electrolyte abnormalities. Stabilization is focused on vigorous rehydration, maintaining urine output, and lowering uric acid levels. Hypercalcemia of malignancy, which is associated with poor outcomes, is treated with aggressive rehydration, intravenous bisphosphonates, and subspecialty consultation. Syndrome of inappropriate antidiuretic hormone should be suspected if a patient with cancer has hyponatremia. This metabolic condition is treated with fluid restriction or hypertonic saline, depending on the speed of development. Febrile neutropenia is one of the most common complications related to cancer treatment, particularly chemotherapy. It usually requires inpatient therapy with rapid administration of empiric antibiotics. Hyperviscosity syndrome may present as spontaneous bleeding and neurologic deficits, and is usually associated with Waldenström macroglobulinemia. Treatment includes plasmapheresis followed by targeted chemotherapy. Structural oncologic emergencies are caused by direct compression of nontumor structures by metastatic disease. Superior vena cava syndrome presents as facial edema with development of collateral venous circulation. Intravascular stenting leads to superior patient outcomes and is used in addition to oncology-directed chemotherapy and radiation therapy. Malignant epidural spinal cord compression is managed in conjunction with neurosurgery, but it is classically treated using steroids and/or surgery and radiation therapy. Malignant pericardial effusion may be treated with pericardiocentesis or a more permanent surgical intervention. Complications of cancer treatment are becoming more varied because of the use of standard and newer immunologic therapies. Palliative care is increasingly appropriate as a part of the team approach for treating patients with cancer.Summary of Oncologic Emergencies
| CONDITION | CANCER ASSOCIATION | COMMON PRESENTING SIGNS AND SYMPTOMS | CONSULTATION CONSIDERATIONS |
|---|---|---|---|
Metabolic
| |||
Tumor lysis syndrome
|
Hematologic malignancies, particularly acute leukemia, and high-grade lymphomas; solid tumors
|
Azotemia, hyperphosphatemia, hyperkalemia, hyperuricemia, acute renal failure, hypocalcemia
|
Oncology, nephrology, palliative care
|
Hypercalcemia of malignancy
|
Multiple myeloma; breast cancer; squamous cell carcinoma of the head or neck, lung, kidney, or cervix
|
Progressive decline in mental function, weakness, anorexia, thirst, constipation, nausea, vomiting, decreased urine output, possible coma
|
Oncology, endocrinology, nephrology
|
Syndrome of inappropriate antidiuretic hormone
|
Small cell lung cancer
|
Hyponatremia, nausea, vomiting, constipation, muscle weakness
|
Oncology, nephrology, palliative care
|
Hematologic
| |||
Febrile neutropenia
|
Current chemotherapy
|
Single axillary/oral temperature ≥ 101.3°F (38.5°C) or sustained temperature ≥ 100.4°F (38°C) for one hour, and an absolute neutrophil count < 500 cells per mm3
|
Oncology, infectious disease, palliative care
|
Hyperviscosity syndrome
|
Waldenström macroglobulinemia (10% to 30%), leukemia, multiple myeloma
|
Spontaneous bleeding, shortness of breath, neurologic deficits (peripheral neuropathies), “sausage-like” hemorrhagic retinal veins, serum viscosity > 4 cP
|
Hematology, oncology
|
Structural
| |||
Superior vena cava syndrome
|
Lung cancer, lymphoma, metastatic mediastinal tumors or lymph nodes, indwelling venous catheters
|
Facial edema, cough, dyspnea at rest, hoarseness, chest and shoulder pain, collateral venous circulation (chest wall)
|
Oncology, cardiothoracic surgery, palliative care
|
Malignant epidural spinal cord compression
|
Breast cancer, multiple myeloma, lymphoma, lung and prostate cancers
|
New-onset back pain (worse when lying down), paraplegia (late presentation)
|
Oncology, neurosurgery, palliative care
|
Malignant pericardial effusions
|
Lung, esophageal, and breast cancers; lymphoma; leukemia; melanoma; infection; treatment complication; autoimmune reaction
|
Dyspnea, chest pain, or palpitations; pulsus paradoxus; Beck triad (muffled heart sounds, hypotension, increased jugular venous pressure)
|
Oncology, cardiothoracic surgery, palliative care
|
Treatment related
| |||
Chemotherapy (extravasations)
|
Current chemotherapy
|
Pain, erythema, and swelling that progress to blanching, blistering, discoloration, and necrosis of the skin
|
Oncology, dermatology, plastic surgery
|
Gastrointestinal problems
|
Current cancer treatment
|
Abdominal pain, nausea, vomiting, diarrhea, constipation, and dehydration; obstruction; bleeding; weight loss; dehydration
|
Oncology, gastroenterology, general surgery, infectious disease, radiology
|
Radiation therapy
|
Current radiation therapy (external, temporary internal, permanent internal, systemic)
|
Dermatitis, cardiovascular disease, esophagitis, cystitis, sexual dysfunction, depression
|
Oncology, dermatology, cardiology, gastroenterology, urology/gynecology
|
Immunotherapy
|
Current immunotherapy
|
Vague symptoms, such as flulike illness and rash
|
Oncology, targeted subspecialty
|
Adapted with permission from Higdon ML, Higdon JA. Treatment of oncologic emergencies. Am Fam Physician. 2006;74(11):1875.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| CLINICAL RECOMMENDATION | EVIDENCE RATING | REFERENCES |
|---|---|---|
Concurrent palliative care consultation should be offered to patients with cancer at the time of diagnosis.
|
C
| |
Emergent use of antibiotics in patients with cancer who present with febrile neutropenia improves survival rates.
|
B
| |
New-onset back pain in patients with cancer should be evaluated as epidural spinal cord compression until it is ruled out.
|
C
| |
More permanent surgical solutions for management of malignant pericardial effusions, such as pericardial windows and indwelling pericardial catheters, are associated with improved patient outcomes compared with percutaneous pericardiocentesis alone.
|
B
| |
Complications from newer immunotherapy treatments often present as nonspecific and vague symptoms, such as flulike illness and rash, requiring a high level of suspicion in patients undergoing cancer treatment.
|
C
|
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
source of the article -https://www.aafp.org/afp/2018/0601/p741.html

pic above svc syndrome

pic above shows the adverse effect of immunotherapy



Comments
Post a Comment